David W. Oaks, psychiatric survivor, speaks a few years ago in Oslo, Norway at a protest.
I do some consulting for the independent nonprofit, MindFreedom International, which is one of the main coalitions focusing on human rights in mental health.
Here are four positive news items about MFI:
1. MindFreedom will be doing another free webinar later this Summer 2018, on choice in mental health.
On August 19, 2018, MindFreedom will be holding a new free online webinar about empowering options for people needing mental and emotional support. The title of the webinar: “Voices for Choices: Organizing for Alternatives to Forced Psychiatric Treatment.”
Thanks to support from the Foundation for Excellence in Mental Health Care, three leaders in the field of providing alternatives to mainstream mental health, will be offering this opportunity. For more information and to register, go here. Act soon, attendance is limited and based on previous webinars, this will be popular.
2. MindFreedom is stronger than ever.
It has been more than five years since I experienced a major accident and severe ongoing disabilities, requiring my retirement after 25 years as MFI’s executive director. As well as the above grant from the Foundation, MFI received an anonymous major donation, and many members have continued to support this important effort.
I am glad to report that MindFreedom International is doing very well. However, there has not been a replacement executive director. Until now. MFI is now announcing a search for a new executive director. This will no doubt lead to better member services, campaigns, and online information, which many people supportive of human rights in mental health have hoped for. Congratulations!
Please note that MindFreedom website currently lists the deadline for the job application as July 31, 2018. So unless this is extended, it is too late to apply.
For more info, see the MindFreedom website here. (Please note that I am not in any way personally involved with the search.)
I have very much enjoyed providing some consulting with MFI through my new business, Aciu Institute. We have helped do several surveys, for example. We look forward to future support for MFI.
3. You can now view MindFreedom’s last webinar, on human rights in mental health, free.
At the beginning of this Summer, 2018, two other psychiatric survivors and I presented a free MFI online gathering about winning campaigns for choice in mental health. You can now view a video recording for free on the web, here.
Above right is a photo of work I did years ago in Oslo, Norway with one of the oldest groups in our movement: We Shall Overcome. We constructed a huge prop hypodermic needle and reaches hundreds in Oslo about choice in mental health. No forced psychiatric drugging!
4. For a limited time, interested activists can apply to benefit from mentorship.
As a follow-up to their webinar MindFreedom International gave about human rights in mental health, about 20 folks can apply to become mentorees. Each will work with a mentor to develop written plans for a human rights in mental health campaign. Because space is limited, those interested should contact MFI soon. Email to: sarah@mindfreedom.org
Go MindFreedom International, go! Let us help lead this revolution!
I am glad to see that MindFreedom International, despite many struggles related to the incredible oppression in the mental health system, and also my accident, is doing so well. Listening to a lot of folks, I know there is hope for a better online presence, member services, etc. But generally these hopes are very constructively and lovingly offered.
Let us all work together for MindFreedom International and the revolution we need in mental health. With the climate crisis, the lock so-called “normality” has on our culture has become a central emergency, globally!
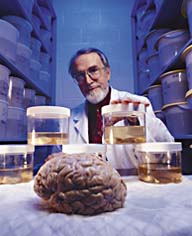
Psychiatrist E. Fuller Torrey promotes court-ordered involuntary psychiatric drugging for millions of Americans. He is winning so many victories that he told NY Times “I feel like I died and went to heaven.”
Many advocates for human rights in the US mental health system already know this sad fact:
The main US government agency that addresses mental health is increasingly under the influence of a special interest group, founded by extremist psychiatrist E. Fuller Torrey. This group, Treatment Advocate Center, promotes court-ordered involuntary outpatient mental health treatment, even if the client lives outside of a psychiatric institution.
However, even after working for decades for human rights in mental health, I have been surprised about how involuntary outpatient ideology is taking over in this government agency, Substance Abuse and Mental Health Services Administration. SAMHSA plans to spend as much as $54 million of US taxpayer money for 17 programs across the country to spread this coercive approach. Four members of a new advisory committee for SAMHSA promote involuntary mental health.
What should be the response from people who care about human rights and mental health?
Sex and Murphy’s Last Law?
The Congress person behind the push for involuntary mental health has been Rep. Tim Murphy (R-PA). Earlier this month, Sept. 2017, mainstream media spotlighted a sex scandal involving Rep. Murphy. It turns out that over the last few years, Rep. Murphy betrayed his wife by hooking up with a volunteer for his horrible mental health legislation. His mistress is also a psychologist, about half his age, and those interested may read a Washington Post article about it here. Of course, the sex life of anyone is their own business, but remember that Rep. Murphy pushes involuntary mental health. Has he had a mental health check-up?
Needless to say, Rep. Murphy’s problems have hurt him on both sides of the aisle.
Of course, involuntary approaches have been a part of the mental health industry for centuries. I oppose all involuntary mental health treatment, because true recovery is based on empowerment. Usually this coercion is behind closed doors inside of locked psychiatric institutions. But since the 1980’s, in the US, state after state has quietly passed mental health laws allowing courts to order people living out in their own neighborhoods to follow mental health treatment, typically psychiatric drugs.
Today, almost all US states practice Involuntary Outpatient Commitment (IOC). Proponents of IOC have found it useful to cover-up this coercion. First, they dropped the word “involuntary.” Then they adopted the mis-named euphemism “Assisted Outpatient Treatment” (AOT).
Assisted?
The movie “Brazil” has an arrest scene in which the subject is “invited to assist” the authorities, and this dark vision accurately describes this kind of “assistance.”
In reality, IOC does not rely on direct physical force. However, knowing that refusal to take your meds will typically result in your immediate detention is extremely coercive.
IOC or AOT, whatever you call it, involves a judge ordering you to follow instructions from your local community mental health system, even if you are law-abiding and living in your own home, peacefully. The special interest group Treatment Advocacy Center (TAC), founded by the psychiatrist E. Fuller Torrey, lobbies for IOC.
TAC cites studies that claim there are 3.9 million Americans with “untreated serious mental illness.” While some of these Americans have a lack of access to mental health care, many simply do not want the traditional mental health treatment, which is often psychiatric drugs. I am one of those who refuses that kind of approach. Are you one of the 3.9 million Americans in the cross hairs of TAC?
TAC Gaining Power in US Government
Kimberly Johnson, PhD, directs the Substance Abuse and Mental Health Services Administration.
This involuntary community treatment seems to be gaining even more authority at SAMHSA, one of the largest mental health agencies on Earth. SAMHSA, led by director Kimberly Johnson, PhD, asked for $4.3 billion in its 2017 budget.
SAMHSA includes the half-billion dollar agency Center for Mental Health Services (CMHS), headed by Paolo del Vecchio. Paolo is one of the few agency heads who publicly discloses that he has lived experience as, his agency calls it, a “mental health consumer.” Until this year, 2017, CMHS has funded the popular Alternatives Conference in the USA, the main place for networking for thousands of mental health consumers since 1985. Apparently this amazingly successful gathering is no longer worth their money, as they find millions for outpatient coerced treatment.
CMHS funds many of the mental health consumer groups in the US. While many of these nonprofits provide important peer support activities, the reliance on CMHS has chilled out and silenced resistance to the rise of dis-empowerment.
Examples of how IOC is gaining influence in SAMHSA:
SAMHSA directs millions in taxpayer money to 17 grant award winners, in a four-year program, that promote IOC, or AOT as they call it. So far, 256 Americans have been included in these programs. According to SAMHSA’s Press Officer Phillip Walls, “The total could go up to about $54 million.”
SAMHSA now has a new Interdepartmental Serious Mental Illness Coordinating Committee’s (ISMICC), to advise it about folks who are considered to have a significant psychiatric disability for a long duration. ISMICC held its first meeting last month, August 2017. I did a simple Google search, and found that four of the 14 members promote involuntary mental health treatment. In fact, one directs TAC.
As I have blogged previously, SAMHSA now has a new position that is popularly called the “mental health czar,” given to psychiatrist Elinore McCance-Katz, who supports AOT.
There is some recent good news. Earlier this month, September 2017, proponents of IOC, or as they call it, AOT, tried to get an extra $5 million per year, which would figure out to more than $20 million dollars over four years. Thankfully, Congress voted this extra money down, 219 to 198 on September 13, 2017. I do not know if money or liberty was the main concern. But if you would like to see how US Representatives voted, go here.
The sex scandal involving Rep. Murphy may be a contributing cause to this failure. Let us hope that the tide is turning for involuntary mental health at SAMSHA.
What Should be Our Response?
Few people know about our little social change movement affectionately called the “Mad Movement.” After centuries of mental health oppression this movement began in about 1969. Quietly, under the radar, some of those who have been through the mental health system, along with supportive allies have worked for human rights and social change in the mental health industry. So what should we do now?
As a survivor of involuntary psychiatry myself, and as a community organizer, my approach tends to be activism.
I worked for MindFreedom International, one of the main independent coalitions in the Mad Movement, for more than 25 years as executive director. Nearly five years ago I experienced a major accident and I retired. Recently, I have acted as a volunteer consultant for MindFreedom with Aciu Institute, a new consulting group I am helping to start with my friend Jeff Bousquet.
Several folks who I respect in the field of mental health empowerment, who bravely survived abuse by their psychiatrists, are funded by SAMSHA directly or indirectly. They have privately told me that they cannot speak out publicly about the rise of involuntary approaches, because of their funding source.
If we are serious, truly serious, about challenging the mental health industry, then we need to develop funding that is independent of that industry. MindFreedom has been one of these groups, refusing to take mental health system money, not that it was offered.
Rise Again!
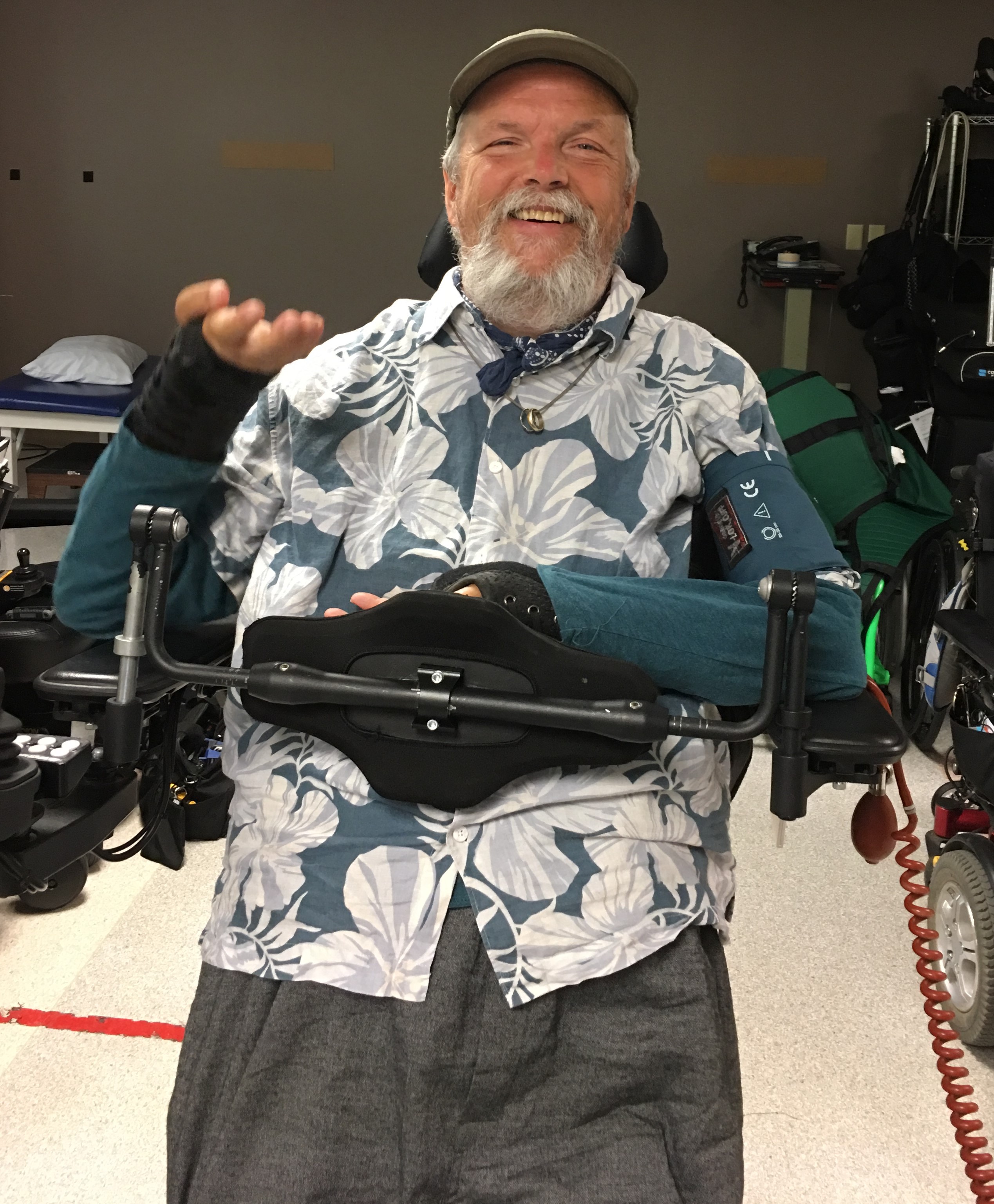
David Oaks tries out a Permobil standing powerchair.
During the past five years, being a quad with a few other disabilities has meant that I have had a bit more time to reflect about our social change movement. Our society seems far too silent in the face of climate crisis. When we should be calling for revolution, it feels like humanity has learned to conform. But let us not give up. Whatever our disabilities, however much SAMSHA is captured by involuntary approaches, and no matter how silent our society is about the climate crisis, fight back! For me personally, one of these ways is that I am looking at a new power chair that can stand me up (see photo).
How can our movement rise now, faced with this push for involuntary mental health? You can leave a public comment on this blog. However, it would be helpful for MindFreedom to get your ideas. We are conducting a survey, and you can indicate if you want your answers to be private or public. I intend to blog about the results. We all want your feedback now! A number of you have already taken this free, brief, private, online survey.
MindFreedom leaders need to hear from folks about their concerns and strategy ideas. Early results show that by far resisting involuntary psychiatric drugging is the most important issue. People taking the survey appreciate MindFreedom’s activism, support for psychiatric survivors, and independence the most.
Below are some of the early survey replies to to the question, “What have you learned or gained from MindFreedom International?”
“I found friends who fight for human rights in mental health.”
“Power to tell my story my way.”
“I gained my life back!!!!!”
“Pride and confidence in my own experience and reality.”
For more information about the MindFreedom survey, contact me, co-founder of Aciu Institute, at davidwoaks@gmail.com.
My Research About SAMSHA
Mr. del Vecchio responded to my email this Spring asking about CMHS support for what is called AOT, and is actually IOC. Whatever it is called, a judge court-orders individuals to follow community mental health instructions. Mr. del Vecchio confirmed by email that this grant program exists, and he sent the list of successful awardees. Below is a copy of his email, with both links to the grant program and the awardees.
To clarify this information, I exchanged email with Mr. Phil Walls, SAMHSA press officer, after a Freedom of Information Act request. Below, you will also find the email from Mr. Walls, confirming that more than $50 million is budgeted for this four-year program with 17 awardees. The only change is that the program for Seattle was cancelled and instead it was redirected to an agency in New Mexico, which just passed an IOC law in 2016.
Delvecchio, Paolo (SAMHSA/CMHS) <Paolo.Delvecchio@samhsa.hhs.gov>
Apr 17 [2017]
COUNTY DEPT OF CMTY & HUMAN SRVS, Seattle WA is no longer a recipient.
But Dona Ana County, New Mexico is now on the list. They receive 700,000/ yr for 4 years.
New Committee Has Several Involuntary Mental Health Proponents
The Interdepartmental Serious Mental Illness Coordinating Committee’s (ISMICC) non-federal membership were selected in August 2017 to serve three-year terms. Their first meeting was held August 31, 2017. Four of those who promote involuntary mental health care include:
Elyn Saks, J.D., Ph.D., Professor of Law, Legal Scholar, University of Southern California Gould School of Law, has a seemingly-complicated position about involuntary treatment. She famously said, “My bottom line? I like to say that I am very pro-psychiatry but very anti-force.” However, she promotes a strange “one-free-shot” philosophy where the mental health system could impose treatment the first time, since she notes some are grateful after the fact. However, others are not grateful. In fact, some do not survive.
John Snook, Esq., Executive Director/Attorney, Treatment Advocacy Center, actually runs TAC and spends his professional career promoting involuntary mental health treatment.
What Is Your Strategy to Respond?
It is OK if circumstances require that you must be private about your resistance to this rise of dis-empowerment at SAMHSA. However, I hope even you do take some kind of action. This is no time for the sidelines.
On this blog comment section, those of you willing to be public may leave your ideas for effective revolution.
And whether or not you are private or public, a member of MindFreedom or not, please take a few moments to fill out this convenient online survey. There is an area for you to indicate whether or not you would like your comments to be public, and if you choose the whole process can be anonymous.
This was from our gathering on Friday, Nov. 4, 2016, at Kesey Square. We visited the office Rep. Peter DeFazio to object to his sponsorship of a bill that would increase coerced psychiatry on an outpatient basis. Left to right on top: Ian, Dale, Sarah, Howard, and that is me sitting down! (Photo by Dale Kegley.)
We are hearing a lot about how the Democratic and Republican parties are so separate. But when it comes to psychiatric survivors, both parties have been willing to throw our folks under a bus. The US Congress simply does not represent us.
Our local alternative newspaper, Eugene Weekly, described our event this way:
International Association for the Advancement of Creative Maladjustment says it hosts a “little peaceful Speak Out Against Psychiatric Dosing” event in Kesey Square 1:30 pm Friday, Nov. 4, 2016. Organizer David Oaks says, “After speakers and an open mic, we will march together to the office of Rep. Pete DeFazio, to object to his co-sponsorship of a bill that would increase outpatient coercion in mental health.” Free.
About a dozen of us held this “Tour” here in Eugene, Oregon to educate the public and our congressperson about human rights and mental health. Unfortunately, Rep. Peter DeFazio (D-OR), who has for decades been a progressive champion of the underdog, has been terribly misinformed, and is a co-sponsor of the worst mental health legislation I have ever seen.
Known as the Murphy Law, thankfully H.R. 2646 has been held up by the US Senate, so far. The worst part of this proposal is that it would give millions of federal taxpayer dollars to support forced outpatient commitment. That is, courts could order Americans living peacefully at home to take psychiatric drugs against their will.
Sarah Smith, MindFreedom, holds the mic for me, David Oaks, at our “tour.” (Photo by David Zupan.)
Incredibly, during a public debate in the “Letters to the Editor” of our Eugene Weekly, Rep. DeFazio not only defended his support, but for the first time in my decades of fighting Involuntary Outpatient Commitment (IOC), he tried to deny that this was mainly about forcing drugs. You may read the three-part published debate between me and Rep. DeFazio here.
What is this bill about, forced hugs? Forced hot chocolate? No, this is about forced drugs of people in their own homes. Frankly, forced hugs and forced hot chocolate are wrong, too. However, I guarantee, along with all the incredible mental health advocacy groups in the USA, that IOC is about the drugs. We have fought these bills on the state level for decades. However, now this is on the federal level, and somehow Rep. DeFazio has been tricked by proponents to believe this has little to do with forced drugs.
Our Tour from Kesey Square to the Federal Building
We started with an ice-breaking introduction at Kesey Square, next to a statue of Ken Kesey, my late friend who authored “One Flew Over the Cuckoo’s Nest.” Among the participants were my friends Dale Kegley and David Zupan. Sarah Smith from MindFreedom was there. One of the main activist labeled autistic, Howard, was there. Psychiatric survivor Gail Roberts was present. Ian McTeague, a young local community organizer, pulled our wagon.
Our “tour” met with a staff person from Rep. Peter DeFazio’s office, who came outside to meet with us. All the security in the Federal Building meant that our group could not get inside. (Photo by David Zupan.)
Several other great activists were there, thanks! Like the cuckoo, we then flew East, on Broadway for a few blocks, to the huge, newish Federal Building. Since security refused to allow us all in, a staff person from Rep. DeFazio’s office came out to meet with us.
For more information about fighting the Murphy bill, and how you need to keep up pressure going into 2017, see my earlier blog entry here.
During our tour on Friday, we chose to deliver our message with humor and positivity. We gave them three awards, assuming “the real” Rep. DeFazio will appear some day and oppose the Murphy Bill. Here is the wording of the three awards:
Award # 1: For Your Future Accomplishment
Award # 1: For Your Future Accomplishment Presented to THE REAL Rep. Peter DeFazio (D-OR). We know the real you: A champion for the powerless. Soon you will see through the Murphy Law, and realize that forced pharma is a key part. Ken Kesey said “Dosing is always wrong!” No forced drugs!
November 4, 2016, International Association for the Advancement of Creative Maladjustment
Award # 2: For Saying “No” to Murphy
Award # 2: For Saying “No” to Murphy Presented to THE REAL Rep. Peter DeFazio (D-OR). Please say to Murphy Law supporters: “If you support forced psychiatry, then you first!” Challenge them to get a mental health check-up first! Tell them that forced psych drugging is the Bill Cosby School of Mental Health.
November 4, 2016, International Association for the Advancement of Creative Maladjustment
Award # 3: The Golden Pill Bottle Award
Award # 3: The Golden Pill Bottle Award. (We affixed a bunch of golden-color pill bottles to the plaque for this one!)
Presented to THE REAL Rep. Peter DeFazio (D-OR). Because you are a skeptic of big corporate power, you can spot the lies of Big Pharma. More than one half of the budget of NAMI comes from drug companies. The Murphy Law is by Big Pharma and would force their drugs!
November 4, 2016, International Association for the Advancement of Creative Maladjustment
If You Live in the Eugene Area?
Please contact the office of Rep. Peter DeFazio by email, now! This just takes a moment. Simply click on this link, and oppose H.R.2646: https://defazio.house.gov/contact/email-me
The Big Pharma Connection
We are glad we discussed NAMI, which is one of the largest mental health advocacy groups. The individual from DeFazio’s office talked about NAMI, but did not know that a Senate investigation revealed that NAMI privately received a majority of its funds from pharmaceutical corporations. For more info about NAMI’s secret source of money, click here for a New York Times article from 2009 that sums up this issue.
The fact that the staff person brought up NAMI is so important, that I have copied the text from this New York Times article:
WASHINGTON — A majority of the donations made to the National Alliance on Mental Illness, one of the nation’s most influential disease advocacy groups, have come from drug makers in recent years, according to Congressional investigators.
The alliance, known as NAMI, has long been criticized for coordinating some of its lobbying efforts with drug makers and for pushing legislation that also benefits industry.
Last spring, Senator Charles E. Grassley, Republican of Iowa, sent letters to the alliance and about a dozen other influential disease and patient advocacy organizations asking about their ties to drug and device makers. The request was part of his investigation into the drug industry’s influence on the practice of medicine.
The mental health alliance, which is hugely influential in many state capitols, has refused for years to disclose specifics of its fund-raising, saying the details were private.
But according to investigators in Mr. Grassley’s office and documents obtained by The New York Times, drug makers from 2006 to 2008 contributed nearly $23 million to the alliance, about three-quarters of its donations.
Even the group’s executive director, Michael Fitzpatrick, said in an interview that the drug companies’ donations were excessive and that things would change.
“For at least the years of ’07, ’08 and ’09, the percentage of money from pharma has been higher than we have wanted it to be,” Mr. Fitzpatrick said.
He promised that the industry’s share of the organization’s fund-raising would drop “significantly” next year.
“I understand that NAMI gets painted as being in the pockets of pharmaceutical companies, and somehow that all we care about is pharmaceuticals,” Mr. Fitzpatrick said. “It’s simply not true.”
Mr. Fitzpatrick said Mr. Grassley’s scrutiny, which he described as understandable given the attention paid to potential conflicts of interest in medicine, had led his organization to begin posting on its Web site the names of companies that donate $5,000 or more. And he predicted that other patient and disease advocacy groups would be prodded by Mr. Grassley’s investigation to do the same.
“Everyone I talk to wants to have more balanced fund-raising,” Mr. Fitzpatrick said.
In a statement, Mr. Grassley praised the alliance for its disclosures. “It’d be good for the system for other patient groups to do what NAMI has done,” he said.
Mr. Grassley’s scrutiny has been unnerving for patient and disease advocacy groups, which are often filled with sincere people who are either afflicted with serious illnesses themselves or have family members who have been affected. Many join the groups in the hope of making sense of their misfortune by helping to find a cure or raising awareness of a disease’s risks and frequency.
Drug makers are natural allies in these pursuits since cures may come out of corporate laboratories and the industry’s money can help finance public service campaigns and fund-raising dinners. But industry critics have long derided some patient organizations as little more than front groups devoted to lobbying on issues that affect industry profits, and few have come under more scrutiny for industry ties than the mental health alliance.
For years, the alliance has fought states’ legislative efforts to limit doctors’ freedom to prescribe drugs, no matter how expensive, to treat mental illness in patients who rely on government health care programs like Medicaid. Some of these medicines routinely top the list of the most expensive drugs that states buy for their poorest patients.
Mr. Fitzpatrick defended these lobbying efforts, saying they were just one of many the organization routinely undertook.
The close ties between the alliance and drug makers were on stark display last week, when the organization held its annual gala at the Andrew W. Mellon Auditorium on Constitution Avenue in Washington. Tickets were $300 each. Before a dinner of roasted red bell pepper soup, beef tenderloin and tilapia, Dr. Stephen H. Feinstein, president of the alliance’s board, thanked Bristol-Myers Squibb, the pharmaceutical company.
“For the past five years, Bristol-Myers has sponsored this dinner at the highest level,” Dr. Feinstein said.
He then introduced Dr. Fred Grossman, chief of neuroscience research at Bristol-Myers, who told the audience that “now, more than ever, our enduring relationship with NAMI must remain strong.”
Documents obtained by The New York Times show that drug makers have over the years given the mental health alliance — along with millions of dollars in donations — direct advice about how to advocate forcefully for issues that affect industry profits. The documents show, for example, that the alliance’s leaders, including Mr. Fitzpatrick, met with AstraZeneca sales executives on Dec. 16, 2003.
Slides from a presentation delivered by the salesmen show that the company urged the alliance to resist state efforts to limit access to mental health drugs.
“Solutions: Play Hard Ball,” one slide was titled. “Hold policy makers accountable for their decisions in media and in election,” it continued.
The alliance’s own slides concluded by saying, “We appreciate AstraZeneca’s strong support of NAMI.”
Mr. Fitzpatrick said that the alliance frequently had such meetings and that the organization would fight for better access to mental health drugs “even if we had no relationship with pharmaceutical companies.”
Tony Jewell, an AstraZeneca spokesman, said that the company was “committed to improving health through partnerships with nonprofit organizations” and that “includes striving to ensure people can access our medicines through formularies managed by state Medicaid agencies.”