Mad In America, major webzine for “rethinking psychiatry,” just published, today, June 29, 2021, my new blog: “Will US Agency New Head End Stonewalling About Money for Involuntary Outpatient Mental Health?” The US Senate confirmed President Biden’s nomination for the new leader of Substance Abuse & Mental Health Services Administration (SAMHSA), Miriam Delphin-Rittmon, PhD, an African-American psychologist.
SAMHSA has been supporting involuntary outpatient mental health, which can mean court-ordering US citizens to take powerful, controversial psych drugs in our own homes in the community. However, SAMHSA has so far refused to provide any information or evaluation about their more than $25 million in grants.
My original Mad In America blog is here, please share & comment:
An audible version of the Mad In America blog is here:
News Updates: Will SAMHSA Start to Repair Damage?
29 June 2021
A few hours before Mad In America published my blog, 29 June 2021, Lindsay Baran, a staff person for the National Council on Independent Living (NCIL), supporting the Mental Health Subcommittee, said:
SAMHSA’s refusal to provide us with the requested information is unacceptable. People are being harmed – their rights are being violated – by these grants, and SAMHSA’s lack of transparency is incredibly alarming.
A few hours AFTER Mad In America published my blog, and I contacted President Biden & SAMHSA, a staff person with SAMHSA’s FOIA office called me at home. She was very nice. She said that there had been quite a turnover in that department. She is the third staff person I am dealing with. She said she had been hired in the Spring, and would get me some materials by this week, or at the latest next week.
This staff person said SAMHSA’s FOIA office had so much material they would need to get it to me as a “rolling” download of about three big files a week. We will let you know about the results.
We will also post other updates here, as we get them. The latest will be on top.
Additional Resources About the SAMHSA Blog
As listed in the blog, July is MAD Pride Month, and you can find out more about it here:
Shortly before my blog was published by Mad In America, I created a personal blog about my experience, including the record heat here in Eugene, Oregon:
Today, Monday, 18 January 2021, we celebrate Rev. Martin Luther King, Jr. In two days, we in the USA will have a brand-new President, thankfully. Every morning I listen to a lot of National Public Radio (NPR). With vaccinations increasing, NPR reported that a “new normality” may finally be possible. A few minutes later, an NPR editorialist warned us, as he should, that the surge of white supremacy must not become a “new normal.”
With all this talk about “new normality,” let me tell you something that MLK wrote and spoke about that is often neglected. MLK called for the end of what we call “normality.” This is my 44th year working for human rights of people with disabilities, so I got very interested when I first heard about this incredible historic fact, and dug in for more.
One of the best examples is that MLK brought a written speech with him in August 1963 to the famous, peaceful March on Washington. At the podium, perhaps after expertly sizing up the huge crowd on the Mall in the summer heat, he never gave that longer written speech. MLK instead improvised, partly based on previous speeches, and gave impromptu what is now known as the “I Have a Dream” speech, one of the most famous in US history.
The title of the original speech that MLK did not give was “NORMALCY — NEVER AGAIN.” This typewritten speech, complete with his corrections marked with xxxxxxx, is carefully archived at the Woodruff Library at Morehouse College in Atlanta, Georgia. Here are some of his words that are most relevant to me today:
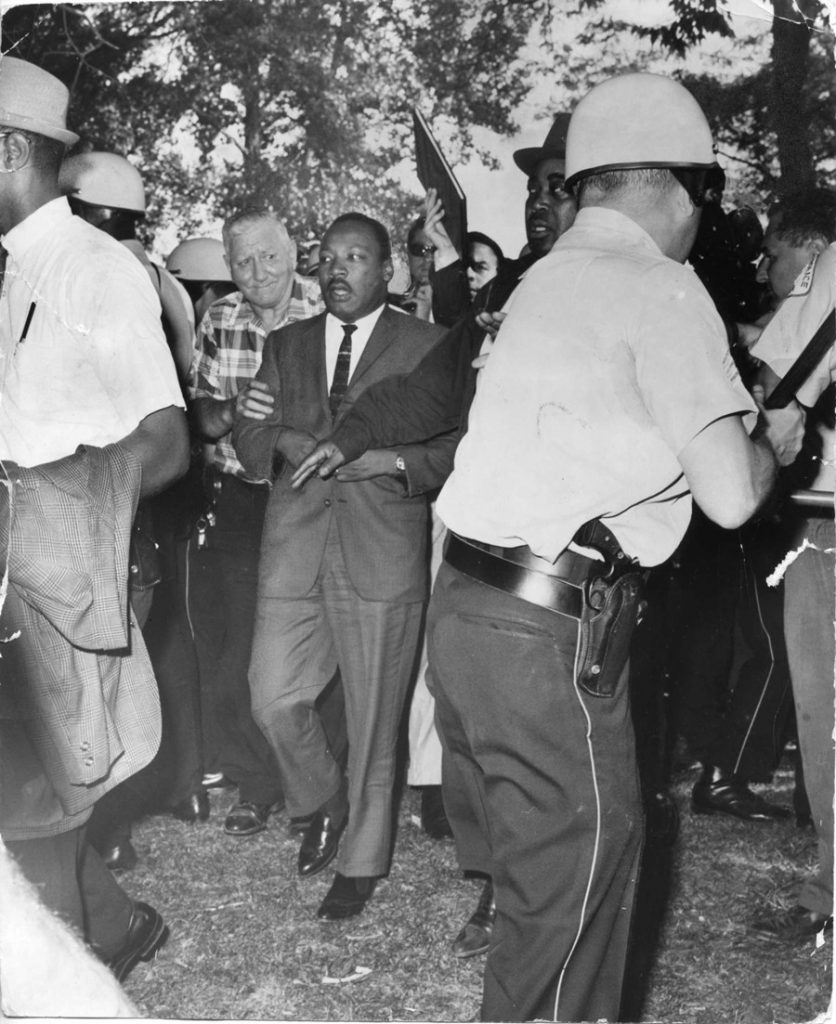
1966: MLK marches on the south side of Chicago, through hundreds of racist counter-protestors.
“[W]e will not be beset by the nagging knowledge that this nation owes an abject apology to Lincoln; an apology for going too slow in granting equal rights to all her citizens; an apology for not pushing hard enough in bringing to reality his hopes and dreams; an apology for invoking the evil alibi that ‘this is not the time’ for the hour of freedom to strike.”
King concluded this part of his speech with words that he would often say other places and are so well put and so important today: “For we know full well that… any time is the time to do the right thing.”
We white USA-born males owe the world an apology for the bigoted folks, mainly white male “citizens,” who are leading the bankrupt ideology of White Supremacy. The best way for us to apologize will be to take action: Black Lives Matter!
MLK frequently visited the theme of challenging normality. He even called for the creation of a “International Association for the Advancement of Creative Maladjustment.” The nonprofit human rights coalition, MindFreedom International, celebrates this vision of having a real IAACM.
Welcome President Joe, But No New Normal!
With the impending inauguration of a new president, many of us feel great relief. Wonderful. But let us learn a lesson from electing President Barack Obama, who I supported. I feel many of us progressives relaxed and let down our guard during Obama’s eight years. Obama himself encouraged progressives to be more active during his administration, and we should have listened to him. Now we know. This time, let us be on guard, prepared, engaged, and always active.
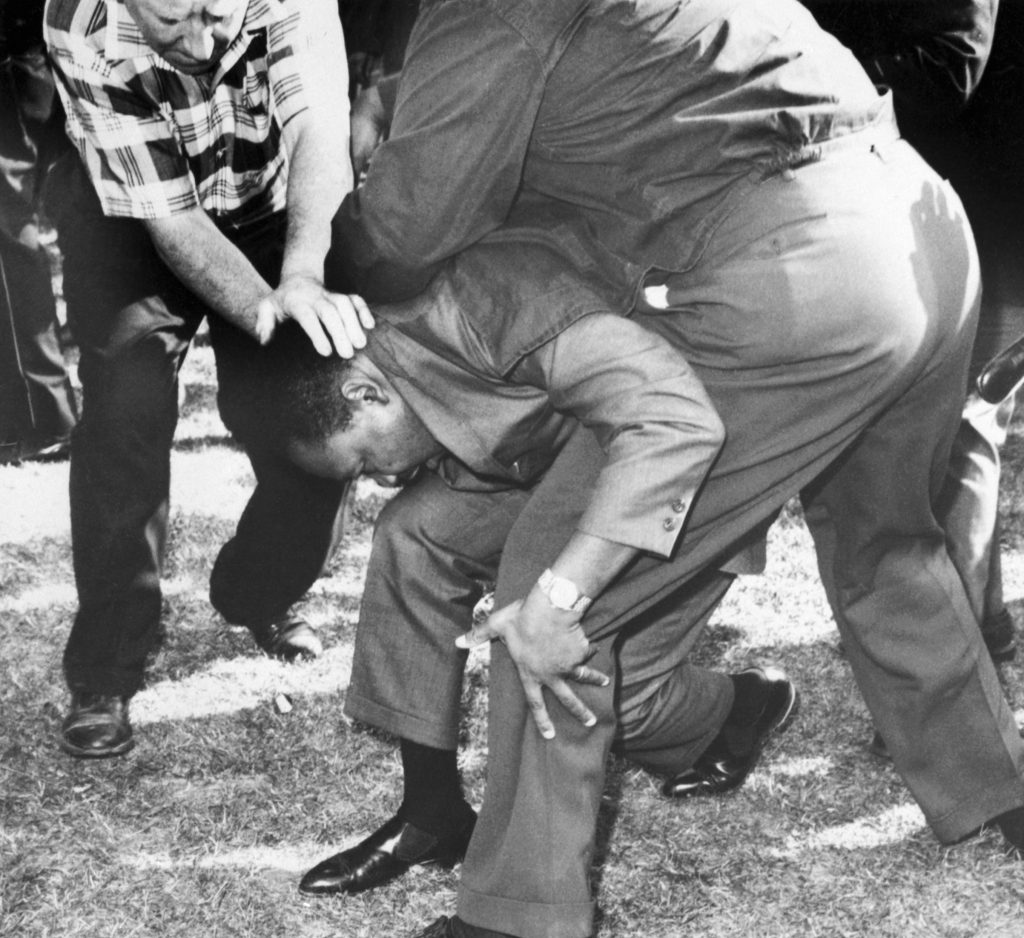
Chicago, 5 August 1966: Struck on the head by a rock thrown by a group of hecklers, Dr. Martin Luther King falls to one knee. Dr. King regained his feet and led a group of marchers.
I think back about my childhood growing up in the south side of Chicago. White Supremacist racism was rampant in that area, not far from the Nazi headquarters. At the age of ten, I was only a few miles away from where Martin Luther King was struck by a rock or brick on 5 August 1966.
I later got out of Chicago, went to college and became a community organizer activist for people with mental or physical disabilities. In 1983, I moved to Eugene, Oregon.
I distinctly remember sitting in Monroe Park, not far from downtown Eugene, Oregon. I was reading material written by MLK. He recalled those days on the south side of Chicago, and I remember he remarked about the intense hate he saw in the eyes of white protestors. MLK said that racists in Mississippi could probably learn from Chicago racists! I especially remember, to paraphrase, that MLK said the hate was so great, his hope was that some young people would get out of the south side of Chicago, go to college, and get away from that environment. I was so startled, it felt like he was writing directly to me.
Perhaps MLK was writing to me, in a sense. Certainly he is speaking to all of us now, that we must never again have “normality.” No normality and no new normality! Ever! Here in our household we even have a little game that you might want to play: Whenever your hear the word “normal” such as on the radio or TV, everyone sneezes or howls. The first to do so “wins.” Let us continue to be allergic to normal or new normal! Why?
Green Disability
Dr. Ellie McCance-Katz, appointed by President Trump to an important mental health position. She resigned in protest 7 January 2021.
On Jan. 7, 2021, the day after the D.C. riots when Trump supporters violently invaded the Capitol, a Trump administration leader for mental health, Elinore McCance‐Katz, M.D., Ph.D., announced her resignation. She had been Trump’s appointed assistant secretary for mental health and substance use at the Substance Abuse and Mental Health Services Administration (SAMHSA).
Yes, we ought to all applaud her resignation in protest of Trump’s rioters. Here is an excerpt from her recent statement:
“I believe that this behavior was totally unacceptable and, in my own heart, I simply am not able to continue. I believe that we are given certain life situations where we must make the difficult decisions and we get one chance to do it the right way.”
However, for the past four years, under Dr. McCance-Katz’s supervision, SAMHSA has sadly betrayed our values in the movement for empowerment of mental health consumers and psychiatric survivors. Quietly, SAMHSA has given two major grants, in 2016 and 2020, to dozens of cities and towns around the USA to support more “court-ordered” coerced mental health care of people living in their own homes out in the community. SAMHSA uses the euphemism “Assisted Outpatient Treatment” (AOT) but really the term that legal scholars use objectively is “Involuntary Outpatient Commitment” (IOC).
We have now made a spreadsheet about grants for outpatient commitment based on SAMHSA’s own public documentation. For more than one year, I requested, unsuccessfully, that SAMHSA supply any reports about the outcome of their support. You may find our spreadsheet about SAMHSA backing of outpatient commitment, as well as a copy of my one year of email dialogue with SAMHSA here:
So, Dr. McCance-Katz, we appreciate your service and your resignation after the white supremacist violence, but please do not reapply for your position at SAMHSA! During your time at SAMHSA, millions were found to support IOC, but SAMHSA claimed poverty when it came to supporting the popular annual Alternatives Conference, which since 1985 has provided a way for hundreds and thousands of US mental health consumers and psychiatric survivors to work together. You can read about the history of Alternatives here:
SAMHSA canceled Alternatives and zeroed out funding support. Now the main annual conference is Peerpocalypse, which is sponsored by a State nonprofit here in Oregon, Mental Health & Addiction Association of Oregon. You can find more about Peerpocalypse here:
It is no surprise and coincidence that the federal agencies who are supposedly working for our mental well-being, instead use coercion to support “normality” and silence the voices of mental health consumers and psychiatric survivors.
SAMHSA is not the only federal mental health agency with a bias toward the old-fashioned medical model approach, and against an empowerment-based model. My friend, psychologist Al Galves, PhD, told me:
My hypothesis is that the National Institute on Mental Health (NIMH) spends more than 80% of its $1.7 billion each year on studying the brain — neural networks, cells, molecules, neurotransmitters, other chemicals and genetics. This is a big problem because human beings don’t use our brains or our genes to live our lives. We use our minds — our thoughts, feelings (emotions), intentions and perceptions to live our lives. The mind is not the same as the brain.
I have often pondered the way so-called “normal” is hurtling itself towards the cliff of environmental catastrophe. Now I realize that humanity as a whole, with a few exceptions such as many indigenous tribes, has a “Green Disability.” That is, it is irrefutable that generally speaking modern humans are so very out of touch with nature, that we threaten our own extinction.
There are five new brief free online videos launched from Greta Thunberg and the Dalai Lama about the role of feedback loops in amplifying the risk of climate crisis. This is why we need immediate and major action, so that seven generations ahead there will still be people and life. Please take a look at these short videos, narrated by Richard Gere:
Our consulting business, Aciu! Institute, has several events and resources for groups fighting to address “green disability.” For more information, click here:
We ought to celebrate today and every day for the liberation movements uplifted by MLK. Yes, many of us will certainly celebrate when the current White House occupant is evicted.
But please, no normality or new normality! Whenever you hear the word “normal,” please join our household and howl or sneeze. We all enjoy our game.
Also, seriously, we need to take real, effective action for a global nonviolent revolution. That is anything but “normal.”
Some of the hundreds of viewers for the David Oaks keynote at Peerpocalypse 2020.
This Summer 2020, I was one of the four keynoters for the major gathering of hundreds of US mental health consumers and psychiatric survivors, Peerpocalypse. Of course, this time it was on Zoom, and at the bottom you can watch my keynote.
Peerpocalypse has a webpage with links to other keynotes, workshops, videos, slides, etc. from the Summer 2020 event. You can view all these for free here: https://www.mhaoforegon.org/2020-conference-slides
Very Few Mad Pride Movement Archives
During the keynote I reference three archives I know about. Here is more information and how to get in touch with them:
U. Mass: My late friend, Judi Chamberlin, is widely acknowledged as one of the main leaders of the start of the Mad Movement. The University of Massachusetts in Amherst received her enormous files of Movement material. These have been catalogued, and you can read more about it here: http://scua.library.umass.edu/umarmot/chamberlin-judi-1944-2010/
OHSU: After I fell in 2012, I helped MindFreedom International donate 23 linear feet of archives to Oregon Health & Science University. OHSU has been busy cataloguing this, and you can read about the archives here: http://archiveswest.orbiscascade.org/ark:/80444/xv71517/
PSAT: Psychiatric Survivor Archives of Toronto gathered a lot of material, and decided to be independent of the university system. I had not heard much about PSAT for a while, so I tracked down board members and exchanged emails. Apparently, they no longer have their web address they used to have. Board member Lucy Costa emailed me in July 2020 that, “Yes, the archives are absolutely safe and secure.” Because of low resources, COVID-19 and questions about issues such as researching Canada’s Archives Act, there has been a lull. Lucy said all is well. You may email them at psychsurvivorarchives@gmail.com.
Incredibly, despite our social change movement doing so much work internationally for so long, these are the only three archives I am aware of. Do you know of any others? My friend, Lauren Tenney, has networked about some artifacts via Facebook. I have not yet seen that, thanks Lauren.
Last year, 2019, we lost a giant in our movement, one of my best friends, Janet Foner. Janet was mainly involved in Re-evaluation Counseling, but strictly separate from that, Janet was also active in co-founding and leading MindFreedom International. Her friend, Lauren Spiro, is in both worlds, RC and what they call the “wide world.” Lauren has edited together a tribute, mainly by RCers (and even though I have never joined RC, they have included my tribute as the only one from the “wide world”). You can read and download here: https://docs.google.com/document/d/1hmVpZ0dfm7jkLUIFb20aA-zA41pOmTNftD9ngCdMzMg/edit?usp=sharing
One of my tributes to fallen leaders is David Heine, a filmmaker and Eugene friend who died fairly recently, 17 July 2020. David created hundreds of documentaries, mainly about art. But he also made some documentaries highly critical of the mental health system. For instance, his younger brother was caught up by involuntary psychiatric drugging for decades, and died early as a result. David made this wonderful documentary about their relationship: “Little Brother Big Pharma.” David also made a movie about alternatives called “Care Farms of the Netherlands.”
Shall We Radicals Network Like We Used To?
During the 1970s & 1980s, for about a decade, radical psychiatric survivors used to gather each Summer, usually on a college campus. These events became known as “International Conference for Human Rights and Against Psychiatric Oppression” (ICHRAPO). I attended several of these but missed the last one in Vermont in 1985. A celebrity visited: Yes, the mayor of Burlington at that time was Bernie Sanders and I understand that he visited and spoke briefly at the International Conference! At about that time, the federal government began funding a big annual conference, so unfortunately Vermont included a lot of acrimony because participants split about how to react to the federal conference. That ended the International Conference.
I have called for restarting the International Conference. Now that people are more familiar with Zoom, we could easily hold a virtual gathering. If you are interested, let me know. Plus, we have started a private group on Facebook and I can get you an invite. Email me at revolution@aciu.info for more information.
Mad Movement Challenges White Supremacy
Yvonne Smith
Several psychiatric survivor activists, including leading African American women such as Celia Brown and Yvonne Smith, have built a network, Surviving Race: The Intersection of Injustice, Disability, and Human Rights, to challenge systemic racism, including connecting with our Mad Movement. Find the Facebook group here: https://www.facebook.com/groups/364074427086419
Federal Support of Coerced Outpatient Mental Health
In my keynote, I referenced how the big federal mental health agency, Substance Abuse & Mental Health Services Administration (SAMHSA) used to fund a popular annual conference of psychiatric survivors and mental health consumers, called Alternatives. SAMHSA has stopped funding such evens, claiming lack of money.
However, SAMHSA found millions of dollars to help promote outpatient coerced mental health treatment. In 2017, I exchanged emails with SAMHSA staff about this, and I included a link to the 17 (since one was dropped, 16) cities: https://davidwoaks.com/samhsa-involuntary-mental-health
UN Leader Calls for “Revolution” in Mental Health
During my keynote, I quoted Special Rapporteur on the Right to Health, at the UN Human Rights Council, Lithuanian Psychiatrist Dainius Pūras, who in 2017 called for a “revolution” because of systemic problems in the mental health system. You can read more here: https://www.ohchr.org/en/NewsEvents/Pages/DisplayNews.aspx?NewsID=21689&LangID=E
Fun On Facebook: Tough Ha! The Last Laugh
Yes, of course we in the USA will be focusing over the next few weeks on de-selecting the incredibly negative current occupant in the White House. In fact, I have created a Facebook group to promote positive dialogue between Trump opponents and those who may have mistakenly voted for him in the past. We need to talk.
I have given this group a slogan, “Tough Ha!” This is the last laugh for by us. I love acronyms, and my acronym for this is TUFFFFHA, which is Trump Unites Family & Friends For Firing His Arrogance (or Ass). I shortened this acronym to TU4FHA. Please do not join this group if you might ever vote for Trump in the future. But everyone else that can hold a civil dialogue, you are welcome to join here: https://www.facebook.com/groups/751355419041364
More About My Consulting Business, Aciu! Institute
During my keynote, I mention Aciu! Institute and some of our videos. I have just blogged about on our Aciu! Institute site. You can go to this link to connect to a whole bunch of videos: https://aciu.info/2020/09/23/david-oaks-peer-keynote-videos/
Peerpocalypse 2020 Workshops & Keynotes
If you missed the Peerpocalypse event, or wish to view any of the workshops or keynotes, they are now all available online, totally free.
Below is an embedded video of my keynote if you would like to watch it right here, about half an hour:
Please click CC above in the lower right of the video then “English” for Closed Captioning to understand my disabled voice more clearly. (If you’ve already started viewing, hover your cursor over the video.)
I already provided a link for the YouTube playlist of the four keynotes for Peerpocalypse 2020. These plus all the dozens of workshops are available free on the Peerpocalypse website, here: https://www.mhaoforegon.org/2020-conference-slides
Aciu to Everyone Who Supported Me For This Keynote!
My wonderful and amazing wife, Debra, helped provide a bit of a laugh track and support during my keynote. Stupendous home care worker, Ian, repeated me and gave wise advice. The staff at Peerpocalypse in Portland were amazing, always responsive to my concerns, taking extra steps for closed captioning, and more. I highly recommend this event, both for viewing the dozens of workshops and other keynotes, and joining with them next year. For more info, click here: https://www.mhaoforegon.org/peerpocalypse-main-page
During my keynote and workshop, we had free ASL interpreting by Patrick Galasso, aciu!
Many other folks have helped me prepare and process the keynote. I would especially like to appreciate the editor for Mad In America, Peter Simons. Just knowing this skilled editor was there was helpful in my work on this blog. And of course, Peter and I exchanged a bunch of communication to finish the MIA blog. Aciu, Peter!
Your Feedback Is Very Much Encouraged & Welcome
On my Mad In America blog, I ended with several ways folks can support the “virality” of my keynote.
In addition, of course, people can comment below on my personal blog. Mad In America gets far more comments on their blog entries and their Facebook. I will also try to watch there and respond.
Psychiatrist E. Fuller Torrey promotes court-ordered involuntary psychiatric drugging for millions of Americans. He is winning so many victories that he told NY Times “I feel like I died and went to heaven.”
Many advocates for human rights in the US mental health system already know this sad fact:
The main US government agency that addresses mental health is increasingly under the influence of a special interest group, founded by extremist psychiatrist E. Fuller Torrey. This group, Treatment Advocate Center, promotes court-ordered involuntary outpatient mental health treatment, even if the client lives outside of a psychiatric institution.
However, even after working for decades for human rights in mental health, I have been surprised about how involuntary outpatient ideology is taking over in this government agency, Substance Abuse and Mental Health Services Administration. SAMHSA plans to spend as much as $54 million of US taxpayer money for 17 programs across the country to spread this coercive approach. Four members of a new advisory committee for SAMHSA promote involuntary mental health.
What should be the response from people who care about human rights and mental health?
Sex and Murphy’s Last Law?
The Congress person behind the push for involuntary mental health has been Rep. Tim Murphy (R-PA). Earlier this month, Sept. 2017, mainstream media spotlighted a sex scandal involving Rep. Murphy. It turns out that over the last few years, Rep. Murphy betrayed his wife by hooking up with a volunteer for his horrible mental health legislation. His mistress is also a psychologist, about half his age, and those interested may read a Washington Post article about it here. Of course, the sex life of anyone is their own business, but remember that Rep. Murphy pushes involuntary mental health. Has he had a mental health check-up?
Needless to say, Rep. Murphy’s problems have hurt him on both sides of the aisle.
Of course, involuntary approaches have been a part of the mental health industry for centuries. I oppose all involuntary mental health treatment, because true recovery is based on empowerment. Usually this coercion is behind closed doors inside of locked psychiatric institutions. But since the 1980’s, in the US, state after state has quietly passed mental health laws allowing courts to order people living out in their own neighborhoods to follow mental health treatment, typically psychiatric drugs.
Today, almost all US states practice Involuntary Outpatient Commitment (IOC). Proponents of IOC have found it useful to cover-up this coercion. First, they dropped the word “involuntary.” Then they adopted the mis-named euphemism “Assisted Outpatient Treatment” (AOT).
Assisted?
The movie “Brazil” has an arrest scene in which the subject is “invited to assist” the authorities, and this dark vision accurately describes this kind of “assistance.”
In reality, IOC does not rely on direct physical force. However, knowing that refusal to take your meds will typically result in your immediate detention is extremely coercive.
IOC or AOT, whatever you call it, involves a judge ordering you to follow instructions from your local community mental health system, even if you are law-abiding and living in your own home, peacefully. The special interest group Treatment Advocacy Center (TAC), founded by the psychiatrist E. Fuller Torrey, lobbies for IOC.
TAC cites studies that claim there are 3.9 million Americans with “untreated serious mental illness.” While some of these Americans have a lack of access to mental health care, many simply do not want the traditional mental health treatment, which is often psychiatric drugs. I am one of those who refuses that kind of approach. Are you one of the 3.9 million Americans in the cross hairs of TAC?
TAC Gaining Power in US Government
Kimberly Johnson, PhD, directs the Substance Abuse and Mental Health Services Administration.
This involuntary community treatment seems to be gaining even more authority at SAMHSA, one of the largest mental health agencies on Earth. SAMHSA, led by director Kimberly Johnson, PhD, asked for $4.3 billion in its 2017 budget.
SAMHSA includes the half-billion dollar agency Center for Mental Health Services (CMHS), headed by Paolo del Vecchio. Paolo is one of the few agency heads who publicly discloses that he has lived experience as, his agency calls it, a “mental health consumer.” Until this year, 2017, CMHS has funded the popular Alternatives Conference in the USA, the main place for networking for thousands of mental health consumers since 1985. Apparently this amazingly successful gathering is no longer worth their money, as they find millions for outpatient coerced treatment.
CMHS funds many of the mental health consumer groups in the US. While many of these nonprofits provide important peer support activities, the reliance on CMHS has chilled out and silenced resistance to the rise of dis-empowerment.
Examples of how IOC is gaining influence in SAMHSA:
SAMHSA directs millions in taxpayer money to 17 grant award winners, in a four-year program, that promote IOC, or AOT as they call it. So far, 256 Americans have been included in these programs. According to SAMHSA’s Press Officer Phillip Walls, “The total could go up to about $54 million.”
SAMHSA now has a new Interdepartmental Serious Mental Illness Coordinating Committee’s (ISMICC), to advise it about folks who are considered to have a significant psychiatric disability for a long duration. ISMICC held its first meeting last month, August 2017. I did a simple Google search, and found that four of the 14 members promote involuntary mental health treatment. In fact, one directs TAC.
As I have blogged previously, SAMHSA now has a new position that is popularly called the “mental health czar,” given to psychiatrist Elinore McCance-Katz, who supports AOT.
There is some recent good news. Earlier this month, September 2017, proponents of IOC, or as they call it, AOT, tried to get an extra $5 million per year, which would figure out to more than $20 million dollars over four years. Thankfully, Congress voted this extra money down, 219 to 198 on September 13, 2017. I do not know if money or liberty was the main concern. But if you would like to see how US Representatives voted, go here.
The sex scandal involving Rep. Murphy may be a contributing cause to this failure. Let us hope that the tide is turning for involuntary mental health at SAMSHA.
What Should be Our Response?
Few people know about our little social change movement affectionately called the “Mad Movement.” After centuries of mental health oppression this movement began in about 1969. Quietly, under the radar, some of those who have been through the mental health system, along with supportive allies have worked for human rights and social change in the mental health industry. So what should we do now?
As a survivor of involuntary psychiatry myself, and as a community organizer, my approach tends to be activism.
I worked for MindFreedom International, one of the main independent coalitions in the Mad Movement, for more than 25 years as executive director. Nearly five years ago I experienced a major accident and I retired. Recently, I have acted as a volunteer consultant for MindFreedom with Aciu Institute, a new consulting group I am helping to start with my friend Jeff Bousquet.
Several folks who I respect in the field of mental health empowerment, who bravely survived abuse by their psychiatrists, are funded by SAMSHA directly or indirectly. They have privately told me that they cannot speak out publicly about the rise of involuntary approaches, because of their funding source.
If we are serious, truly serious, about challenging the mental health industry, then we need to develop funding that is independent of that industry. MindFreedom has been one of these groups, refusing to take mental health system money, not that it was offered.
Rise Again!
David Oaks tries out a Permobil standing powerchair.
During the past five years, being a quad with a few other disabilities has meant that I have had a bit more time to reflect about our social change movement. Our society seems far too silent in the face of climate crisis. When we should be calling for revolution, it feels like humanity has learned to conform. But let us not give up. Whatever our disabilities, however much SAMSHA is captured by involuntary approaches, and no matter how silent our society is about the climate crisis, fight back! For me personally, one of these ways is that I am looking at a new power chair that can stand me up (see photo).
How can our movement rise now, faced with this push for involuntary mental health? You can leave a public comment on this blog. However, it would be helpful for MindFreedom to get your ideas. We are conducting a survey, and you can indicate if you want your answers to be private or public. I intend to blog about the results. We all want your feedback now! A number of you have already taken this free, brief, private, online survey.
MindFreedom leaders need to hear from folks about their concerns and strategy ideas. Early results show that by far resisting involuntary psychiatric drugging is the most important issue. People taking the survey appreciate MindFreedom’s activism, support for psychiatric survivors, and independence the most.
Below are some of the early survey replies to to the question, “What have you learned or gained from MindFreedom International?”
“I found friends who fight for human rights in mental health.”
“Power to tell my story my way.”
“I gained my life back!!!!!”
“Pride and confidence in my own experience and reality.”
For more information about the MindFreedom survey, contact me, co-founder of Aciu Institute, at davidwoaks@gmail.com.
My Research About SAMSHA
Mr. del Vecchio responded to my email this Spring asking about CMHS support for what is called AOT, and is actually IOC. Whatever it is called, a judge court-orders individuals to follow community mental health instructions. Mr. del Vecchio confirmed by email that this grant program exists, and he sent the list of successful awardees. Below is a copy of his email, with both links to the grant program and the awardees.
To clarify this information, I exchanged email with Mr. Phil Walls, SAMHSA press officer, after a Freedom of Information Act request. Below, you will also find the email from Mr. Walls, confirming that more than $50 million is budgeted for this four-year program with 17 awardees. The only change is that the program for Seattle was cancelled and instead it was redirected to an agency in New Mexico, which just passed an IOC law in 2016.
Delvecchio, Paolo (SAMHSA/CMHS) <Paolo.Delvecchio@samhsa.hhs.gov>
Apr 17 [2017]
COUNTY DEPT OF CMTY & HUMAN SRVS, Seattle WA is no longer a recipient.
But Dona Ana County, New Mexico is now on the list. They receive 700,000/ yr for 4 years.
New Committee Has Several Involuntary Mental Health Proponents
The Interdepartmental Serious Mental Illness Coordinating Committee’s (ISMICC) non-federal membership were selected in August 2017 to serve three-year terms. Their first meeting was held August 31, 2017. Four of those who promote involuntary mental health care include:
Elyn Saks, J.D., Ph.D., Professor of Law, Legal Scholar, University of Southern California Gould School of Law, has a seemingly-complicated position about involuntary treatment. She famously said, “My bottom line? I like to say that I am very pro-psychiatry but very anti-force.” However, she promotes a strange “one-free-shot” philosophy where the mental health system could impose treatment the first time, since she notes some are grateful after the fact. However, others are not grateful. In fact, some do not survive.
John Snook, Esq., Executive Director/Attorney, Treatment Advocacy Center, actually runs TAC and spends his professional career promoting involuntary mental health treatment.
What Is Your Strategy to Respond?
It is OK if circumstances require that you must be private about your resistance to this rise of dis-empowerment at SAMHSA. However, I hope even you do take some kind of action. This is no time for the sidelines.
On this blog comment section, those of you willing to be public may leave your ideas for effective revolution.
And whether or not you are private or public, a member of MindFreedom or not, please take a few moments to fill out this convenient online survey. There is an area for you to indicate whether or not you would like your comments to be public, and if you choose the whole process can be anonymous.
A US Senate committee is supposed to approve a controversial Trump appointee this Tuesday, 1 August 2017. You may not have heard about this in mainstream media, or even the alternative media, though I have been covering this topic for months!
The approval ceremony is scheduled for streaming on the US Senate HELP (Health Education Labor Pensions) Committee website. According to what I have heard, this HELP Committee will genuflect to power, and sign off on the appointment of psychiatrist Dr. Ellie McCance-Katz as the first Assistant Secretary of Substance Abuse and Mental Health Services Administration (SAMHSA), a powerful federal agency with a budget close to four billion dollars annually.
This new “Mental Health Czar,” as it is popularly known, will preside over a SAMHSA that is supposed to be far more friendly to the mental health industry. For example, several leaders have said that SAMHSA will not fund the popular Alternatives Conference after August 2017 in Boston. For more than three decades, this annual gathering has brought together countless USA psychiatric survivors and mental health consumers who lead hundreds of empowering peer recovery programs.
For the past few years, SAMHSA has even begun to fund the support of Involuntary Outpatient Commitment, which often translates into court-ordered coercive psychiatric drugging of people living in their own homes, peacefully. All the groups I know led by people who have been through the mental health system strongly oppose IOC.
Dr. Ellie McCance-Katz, appointed by President Trump to a important mental health position.
I just heard from leaders at the National Council on Independent Living (NCIL) that this apparently-automatic approval can be watched this Tuesday, 1 August 2017; the link will go live about 15 minutes before the hearing, set for 2:30 EST:
It is not too late to speak out to your US Senators, especially if one is on the HELP Committee. Suggest that the HELP Committee ask Dr. McCance-Katz some tough questions.
More information about this important yet quiet appointment can be read on my blog:
2. Send a web note to each Senator, it takes just a moment: “I oppose the Trump nomination for the new, powerful mental health position, Assistant Secretary to SAMSHA. The US Senate HELP Committee is supposed to ask psychiatrist Dr. Ellie McCance-Katz questions, here are nine questions:
3. Add your own questions, if any. Copy and post your message, so we all know you speak out for human rights!
4. If your US Senator is on the Senate HELP (Health Education Labor Pensions) Committee, you have extra weight. The list of members is here: https://www.help.senate.gov/about/members
5. For extra, phone up your US Senators. They have both local and D.C. offices. Get to know the staff people who work on health by their first name.
6. Spread the word via email, FB, comments on blogs, Twitter, etc.
Dr. Ellie McCance-Katz, appointed by President Trump to a important mental health position.
Next week should be interesting, perhaps revolutionary, for those of us who care about human rights, disability and mental health.
I heard from leaders at the National Council for Independent Living (NCIL) that the US Senate HELP Committee will be quizzing Pres. Trump’s appointment psychiatrist Dr. Ellie McCance-Katz, to a new powerful mental health position in the federal government.
This new job is commonly known now as “Mental Health Czar” and if you are new to this little-known controversy, I blogged about this a few days ago.
9 Questions that Should Be Asked that Haven’t Been
Technically, Dr. McCance-Katz is being recommended by Pres. Trump to be Assistant Secretary for the huge USA Substance Abuse and Mental Health Administration (SAMHSA). Mental health agencies mainly are asking about her positions regarding “recovery” and “peers,” important topics, but here are some tougher questions:
Do you support or oppose SAMHSA Involuntary Outpatient Commitment (IOC), such as court-ordered coerced psychiatric drugging? (Yes, in the last few years, some of your US taxpayer millions have gone to support court-ordered psychiatric procedures, mainly to enforce involuntary drugging. This has been done for decades by laws changing quietly on the state level. Now your USA federal government has thrown its weight behind this atrocity.)
If you do support this, then about how many more million Americans do you feel should get court-ordered drugging? (Fanatics for IOC, which they call Assisted Treatment to hide what it really does, are a bit shy about the number of Americans they would like to see involuntarily drugged.)
Do you endorse the current use of federal money for IOC? (Let us hear about how many millions have already been spent by federal agencies to promote IOC. Easy enough to find out. How many more millions are planned for, how many more millions would Dr. McCance-Katz want?)
Do you admit that court-ordered involuntary electroshock on an outpatient basis can be done? (Find this incredible? Very occasionally, on the state level, IOC has reached the bizarre extreme of court-ordered involuntary outpatient electroshock. Where the subject has to report regularly to a local hospital for another forced outpatient electroshock, or face re-institutionalization. For more proof, use your web search engine for these phrases: ray sandford electroshock, elizabeth ellis electroshock. An attorney confirmed federal support for IOC could conceivably mean more forced outpatient electroshock. Even one more American forced shock is wrong. Outpatient forced shock is horrible. So is inpatient forced shock, which has gone on continuously in the USA and most countries, for decades including now!)
What is the long-term impact of psychiatric drugs?
Did you know that neuroleptic psychiatric drugs, commonly called antipsychotics, are often used during IOC?
Did you know infants and children in the USA and globally are given off-label neuroleptics?
Did you know these drugs are well known to cause brain damage, such as tardive dyskinesia (easily viewed on Youtube) or an actual lobotomy effect, shrinking the frontal lobes?
Why aren’t non-drug alternatives offered to Americans, including the millions of vets?
And many other questions!
You may suggest more questions here on the comment section. Sometimes my blog entries are picked up by the big website Mad in America. Incredibly, my last blog about this topic led to a flurry of predictable controversy about Hillary vs. Trump vs. whoever.
Look, this is far deeper than who is in the White House. Whether it is Pres. Pence or the signer of the 21st Century Cures act, one of his last acts as President, Barack Obama (and I generally support him), can we discuss that later?
Whether you are Republican, Democrat, Libertarian (which has had a plank for years against government forced psychiatry, of course), a Berniecrat, Green, whatever, okay. For more than 40 years I have worked for human rights and mental health. I have seen Americans and people from other countries of all political stripes speak up. For example, we psychiatric survivors warned about the undo power of the drug industry to SAMHSA, in 2010.
Come on, especially we who are survivors of psychiatric coercion! Let us have a revolution. Certainly no one can stop us for speaking up with the truth!
Mad with the truth!
Speak out against this violation, speak out for freedom!
NCIL is holding their annual conference during this same week that the US Senate should be asking tough questions. NCIL’s theme is Revolution.
The last time I was able to attend this great conference, I heard one of the last speeches from my late, departed friend Justin Dart, Jr., known as the father of the ADA. Justin called for revolution, and both he and his amazing widow have known that psychiatric survivors tend to have the fire in our bellies for freedom, love, and revolution!
Dr. Ellie McCance-Katz, appointed by President Trump to a important mental health position.
I am a survivor of human rights violations in the mental health system. And even though this was a long time ago, back when I was a college student in the 1970’s, the issues are more relevant than ever. My friend, Patch Adams, MD, has connected the dots for me: Our society needs to be very agile right now, but has to overcome centuries of mental health oppression. But with compassion, we can have a global nonviolent revolution!
Recent events show that mental health human rights violations are important for everyone. MindFreedom International was my employer for 25 years before my accident in 2012. They are an independent, activist group, and we need that energy as never before.
The White House announced this past Friday, 21 April 2017, in the evening, that President Donald Trump has, for a pivotal mental health position, appointed a psychiatrist who openly speaks out for involuntary psychiatric drugging of people living outside of institutions, even in their own homes. This appointee criticizes our social change movement, especially our dedication to empowering peer support and our concerns about psychiatric drugs and labeling. It is important for everyone who supports human rights, especially in the social change movements for disability rights and those critical of mass incarceration, to speak up and oppose this approach.
Please phone your U.S. Senators to block this confirmation. This is a chance to raise these issues, now!
This “Assisted Outpatient Treatment” (as supporters call it) or “Involuntary Outpatient Commitment” (as it is known by many) has been quietly growing on the State level for decades, but is now being funded on the federal level, such as through the enormous 21st Century Cures Act that was passed by Congress at the end of last year. Whatever it is called — AOT or IOC — under these laws judges may order folks to have mental health care, which could be a range of approaches. In my experience, staffing a human rights phone and getting hundreds of contacts for decades, “mental healthcare” for the “seriously mentally ill” almost always includes psychiatric drugging, often with neuroleptics, or “antipsychotic medications” as prescribers often call this family of pharmaceuticals.
Neuroleptic drugs began in the 1950’s with such brands as Thorazine, Stelazine, Haldol, Mellaril, etc., all of which I have had. I personally experienced involuntary neuroleptic injections more than 40 years ago as a college student at Harvard. About five times I was placed in a psychiatric institution for emotional difficulties, and twice I experienced the sharp end of a needle, when in solitary confinement I was held down on the bare mattress and got forced drugging in my butt. I graduated anyway, in 1977, and our class is celebrating its 40th anniversary this year.
Now neuroleptics have dozens of more brands, but many of the hazards and risks are the same. For instance, in the long run there is the danger that many people can experience involuntary twitching that can apparently often be permanent. There is also the long term risk of brain damage and even death. Some folks choose these medications, but others do not. I choose to not take them, and I have not for these past four decades.
Takes One to Know One
President Trump has appointed Dr. Ellie McCance-Katz for a high-level position created by the 21st Century Cures Act. Dr. McCance-Katz would become the first Assistant Secretary for Mental Health and Substance Abuse (SAMHSA) inside the federal Department of Health and Human Services.
In an essay published last year by the Psychiatric Times, Dr. McCance-Katz was highly critical of SAMHSA, especially its sub-agency Center for Mental Health Services (CMHS), headed by Paolo Delvecchio, who has long-identified himself as an individual who has used psychiatric treatment. Many mental health consumers and psychiatric survivors know Paolo because of his work in this field for decades.
In her essay in Psychiatric Times, Dr. McCance-Katz:
Endorses federal funding of AOT (or IOC).
Criticizes SAMHSA for allegedly being critical of psychiatric drugs.
Challenges the support for “recovery” in mental health, a term used by many consumer/survivors as a rallying point for hope and empowerment.
Calls for mental health care, which appears to be led by psychiatric drugs, for more than three million Americans.
Are You One of the Many Targeted?
Dr. McCance-Katz wrote in the essay: “It is estimated that 10 million Americans (4.2%) are living with serious mental illness. However, only 68.5% of the most severely mentally ill will receive any type of mental health services.”
I wonder how many of these three million Americans would refuse psychiatric drugs? Of those who would refuse, I wonder how many this psychiatrist would like to see drugged against their will?
This professor challenges the great interest in using peer support as a humane, empowering alternative priority. She writes, “Workforce issues focus in large part on the development of a ‘peer workforce.’ This ideology purports that one can become a mental health professional by virtue of having a mental illness. Peer support can be an important resource for some, but it is not the answer to the treatment needs of the seriously mentally ill.”
There are only a few, small groups that focus on involuntary psychiatric drugging, such as the Treatment Advocacy Center. The topic actually divides a lot of folks, since the average American in my experience does not like the idea of the government forcing citizens to have involuntary psychiatric drugs, once the value of empowering alternatives are explained. IOC can even for a small group include involuntary outpatient court-ordered electroshock, or electro-convulsive therapy (ECT). For example, search the web for the names Ray Sandford and Elizabeth Ellis, with the word electroshock. These two Minnesotans who received such horrible involuntary procedures, but MindFreedom put out human rights alerts that stopped the series of electroshocks.
In my decades of work in the field of human rights and mental health, I have been impressed with the way concern about this issue crosses political lines. Yes, support for this field has often been among those who would be seen as on the left. However, some of the most effective organizing about psychiatric over-drugging of children has been done by activists that would be seen as on the right.
I have seen both the Libertarian Party and the Green Party both pass planks in their platform, years ago, expressing support for some of our goals. Today we are often seeing critics question the sanity of the President of the United States because of his support of untrue beliefs, such as his denial of climate crisis and his many years of championing the odd belief that President Obama was born in Africa.
Well, it takes one to know one, and I am also a White Aging Crazy Citizen (WACC). Actually, what I have found in my work is that 100% of all people struggle about their mental wellness, it is a universal challenge. The distinction is between negative, bigoted craziness and positive, constructive, creative craziness. In fact, I would argue that the new PC is Positively Crazy.
Perhaps at this time, we need a Positively Crazy dedication to the First Amendment, which not only includes free speech, but according to the US Supreme Court, the right to think unusual thoughts, even irrationally. There are more compassionate, effective, sustainable ways to help troubled people. Let us all break the silence about human rights violations in mental healthcare, including IOC. Centuries of abuse in this industry have helped silence the population on many outrages, including the threat of climate chaos.
We need a nonviolent revolution throughout our society, in mental healthcare, in energy, in so many ways. There is no guarantee of results, but at least we can speak up about freedom!
My friend Patch Adams, MD has spoken out many time about the need for fun, creativity and peaceful rebellion. You may read a recent blog I wrote after chatting with him recently, which you may read here
End
Below, for the very interested, you will find an essay I have just submitted to be published in the Harvard Alumni Association publication that comes out every five years. In my essay, I appreciate that a Harvard volunteer group first placed me as an intern working for human rights in mental health. Unfortunately, the nonviolent revolution we have long called for in mental health has not quite happened yet. However, perhaps now this topic may get more attention.
My Essay to Harvard Alumni Association for My 40th Reunion
Mental health. Activism. Community organizing. Human rights. Disability. Nonviolent revolution! Thank you, Phillips Brooks House Association, for placing me as an intern in my senior year as a community organizer of people in the mental health system, because the above passions became my career. The incredible riches I have gained from working with some of the most powerless in our society are invaluable. After 25 years as Executive Director of the human rights nonprofit MindFreedom International, I had an extreme accident and broke my neck, and I now use a power chair. While it would be impossible to be totally prepared for this, my work in the disability movement managed to teach me a few principles. For example, I apply lessons from Martin Luther King, Jr.: What is my creative maladjustment?
Reflecting back on Harvard, the most memorable and influential class for me was about comparative religion. It would be fun to be in touch with any of you reading this. You can find me easily by directing your search engine to this phrase: david w oaks blog. When I summarized my passions above, I included “nonviolent revolution.” Yes, for decades I have raised this as a real choice. Now, with the climate chaos looming, I feel nonviolent revolution is an option we might want to choose. Scientists have estimated that the lag for carbon-induced impact is about 40 years. In other words, the pollution during our years at Harvard is only now changing the climate. I am very concerned that during the next lag, many more feedback effects can be triggered. For the current moment and for seven generations in the future, we truly need a nonviolent revolution. I estimate seven generations would extend to about the year 2192. May there be a healthy graduating class that year! The Butterfly Effect gives us a good chance, uncertain, but a good chance. Perhaps it is up to you?
It is important to create a dialogue to address the values we need today for excellent care. Therefore, I am copying the commentary that I very much disagree with. You may read the essay by the Trump appointee from Psychiatric Times below:
The Federal Government Ignores the Treatment Needs of Americans With Serious Mental Illness
By Dr. Ellie McCance-Katz
There she was again—a middle-aged woman, disheveled, crouching in the doorway of a closed store, grasping a notebook and pencil and scribbling. Intermittently, her eyes darted around and she would mumble, then go back to her notebook. Her eyes never met mine, but I wondered why she was not getting help with what was clearly a severe mental illness. I would see her in that same doorway several times a week for a couple of years before I left Berkeley, California, to become the first Chief Medical Officer of the Substance Abuse and Mental Health Services Administration (SAMHSA). In doing so, I hoped to help people living in the grips of cruel disorders that affect one’s thinking, one’s reasoning, one’s ability to relate, and one’s ability to even understand that one suffers from a disorder that can be treated.
It is estimated that 10 million Americans (4.2%) are living with serious mental illness. However, only 68.5% of the most severely mentally ill will receive any type of mental health services. Whether those services are necessary and appropriate is not known. People with schizophrenia, bipolar disorder, depression, and other severe mental illnesses often complicated by substance misuse need effective, safe, evidence-based treatments as well as community resources where their clinical service needs can be met. The federal Department of Health and Human Services (HHS) is composed of numerous agencies that address the health care needs of Americans, but only one agency within HHS is charged with addressing the needs of those with serious mental illness and that is SAMHSA.
SAMHSA is a small federal agency with a budget of roughly $3.7 billion per year; much of that is in the form of block grants to states that are the arbiters of how the funds will be spent in support of the treatment of substance use and mental disorders. SAMHSA does, however, have the ability to focus on areas and issues that would improve the lot of individuals affected by severe mental illness. Unfortunately, SAMHSA does not address the treatment needs of the most vulnerable in our society. Rather, the unit within SAMHSA charged with addressing these disorders, the Center for Mental Health Services, chooses to focus on its own definition of “recovery,” which generally ignores the treatment of mental disorders, and, as a major initiative under “recovery” services, focuses on the development of a “peer workforce.”
There is a perceptible hostility toward psychiatric medicine: a resistance to addressing the treatment needs of those with serious mental illness and a questioning by some at SAMHSA as to whether mental disorders even exist—for example, is psychosis just a “different way of thinking for some experiencing stress?”
SAMHSA’s approach includes a focus on activities that don’t directly assist those who have serious mental illness. These include programs such as Mental Health First Aid, which seeks to teach people about the warning signs of mental illness in an attempt to provide support to those who are experiencing symptoms. Significant dollars are spent on hot lines for callers who may be experiencing suicidal thinking or who know someone who may be—yet suicide rates continue to climb in the US. SAMHSA supports integrated care programs that would bring some aspects of primary care to mental health services programs—worthy programs, but which do not address the treatment of serious mental illness. Programs that undertake the “re-education” of mental health practitioners who are assumed to be abusers of “consumer” rights and who dictate treatment to patients have been funded in the Recovery to Practice initiative.
Workforce issues focus in large part on the development of a “peer workforce.” This ideology purports that one can become a mental health professional by virtue of having a mental illness. Peer support can be an important resource for some, but it is not the answer to the treatment needs of the seriously mentally ill.
Lost in all of this are the real and pressing treatment needs of some of the most vulnerable in our society—those living with serious mental illness. Nowhere in SAMHSA’s strategic initiatives is psychiatric treatment of mental illness a priority. The occasional vague reference to treatment is no substitute for the urgent need for programs that address these issues.
What’s needed?
What is needed is an agency soul-searching and a re-prioritization that places the treatment of serious mental disorders at the very top of the list of agency goals. SAMHSA needs leadership that acknowledges the importance of addressing serious mental illness. Initiatives that provide funding for new approaches to engaging the seriously mentally ill; for assisted outpatient treatment with enriched psychosocial services; and for additional psychiatric hospital beds, particularly for longer-term care given the severe shortage of such resources in the US, should be at the top of SAMHSA’s agenda.
Clinical education programs that address current, evidence-based treatment for serious mental illness, and new funding for the training of mental health professionals, including psychiatrists, advanced practice psychiatric nurses, and psychologists, should be a major focus. SAMHSA should develop closer ties with the National Institute of Mental Health, which is helping us to better understand the neurobiological underpinnings of mental illness every day. The real hope, change and ability to recover from these disorders, lies in their effective treatment. To ignore this is to leave a large segment of some of the most seriously ill in our society abandoned—indeed, discriminated against by the very agency charged with serving them.
What can be done to change the current course? Stakeholder groups that seek to ensure psychiatric treatment for all who need it should band together and exert pressure on SAMHSA, on political administrations, and on congressional representatives to address the needs of the seriously mentally ill. Skilled behavioral health providers with patient care experience—psychiatrists, psychologists, social workers, counselors—should consider committing a period of service to SAMHSA and to other federal agencies to inform policy decisions related to substance use and mental disorders. This is especially important because too many in the government have education in behavioral health fields but have never worked with patients, or if they have, it was many years in the past. Being inside the Beltway also imbues an artificial perspective that may be informed by lobbyists if at all. This does not serve the American people.
Time for change
I left SAMHSA after 2 years. It became increasingly uncomfortable to be associated with an agency that, for the most part, refused to support evidence-based psychiatric treatment of mental disorders. It was also quite clear that the psychiatric perspective I brought—inclusive of assessment, diagnosis of mental disorders, utilization of evidence-based treatments, including psychotropic medication and psychosocial interventions as integral components of recovery—was a poor fit for the agency. SAMHSA needs a complete review and overhaul of its current mission, leadership, and funded programs. Congress should quickly address this through legislative mandate.
For too long the treatment needs of the seriously mentally ill have been ignored by SAMHSA, and this needs to change. In doing so, perhaps people like the woman in the doorway will be able to move out of the shadows to live full and productive lives in our communities.